Causes
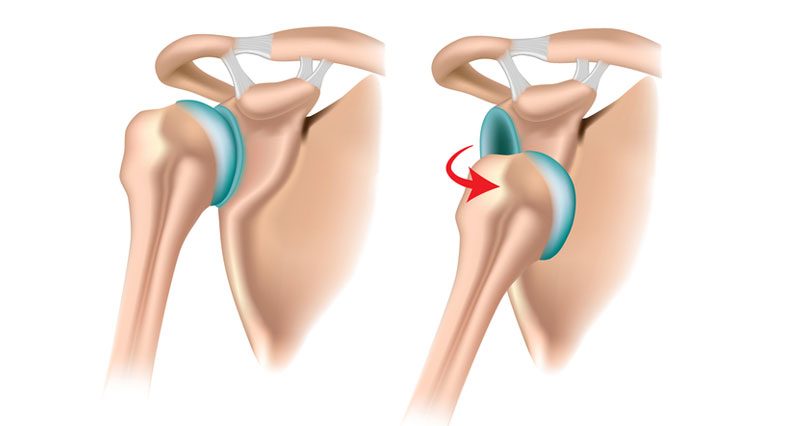
The glenohumeral joint is a ball and socket joint that has the greatest range of motion with the least stability. When a dislocation occurs, the ball and socket of the shoulder separates. There is a difference between a subluxation, the joint spontaneously reduces, and a dislocation; an emergency situation to have assistance to reduce the joint. When recurrent instability events occur, the glenohumeral joint moves in and out of the socket (glenoid) in any direction, causing damage. The certain type of damage dictates certain types of solutions or treatments.
Shoulder dislocation common symptoms:
(1) intense pain
(2) Numbness or tingling
(3) “Popping sensation”
(4) An Inability to move the arm
(5) Loss of range of motion
(6) An obvious deformity
Diagnosis
Most glenohumeral instability events occur in patients under the age of 25 years old and have the greatest probability of a recurrent event. Patients over the age of 25 can still have first time instability events, but are more likely to rehabilitate their injury with conservative treatment. Dr. Nicholson will evaluate the shoulder in the office with a clinical exam. X-rays or other diagnostic tests may be recommended to further evaluate the joint.

Non-Surgical Treatment
Non-surgical treatment goal is to reduce pain, restore range of motion and create stability. Many patients with dislocation injury benefit from conservative management.
Rest: Resting the injured joint is the first step to reduce swelling and pain. Keeping it immobilized for the first 2-5 days will help with pain. Be sure to use the arm gently within a week to avoid a frozen shoulder.
Ice: In the first 24 hours of an injury, ice it to reduce swelling and pain.
Heat: After 24 hours have passed, a heating pad or hot compress can help.
NSAIDS (non-steroidal anti-inflammatory drugs): Reduce pain and swelling through NSAIDS such as ibuprofen (Advil), naproxen (Aleve), or aspirin.
Physical therapy and exercise: Gentle exercises and stretches designed to strengthen the muscles surrounding the shoulder joint.
Surgical Treatment
Surgical treatment is recommended for patients who did not benefit from non-surgical management. With recurrent instability events, Dr. Nicholson may recommend an arthroscopic instability repair. This may involve a labral repair or tightening the capsule, called a “capsulorrhaphy”. This is commonly an arthroscopic outpatient procedure.
Patients can expect to wear a sling for 4-6 weeks and attend formal physical therapy for 8-16 weeks. Athletes can expect to return to non-contact sport between 4-5 months and contact or collision sport between 5-6 months.